These notes are based on a wonderful lecture I had today titled 'quality improvement in health care pathways'. It was a short lecture full of simple but powerful ideas.
I am quite fortunate that my hospital is modern and has a lot of money. One of the ways the administration has decided to spend this money is on a 'quality care' unit whose job is simply to improve patient outcomes and increase the 'quality' of care.
Quality is notoriously difficult in healthcare to measure. The main way that quality is measured in most institutions is by comparison to local and national mortality and infection rates. Yet these gives you no idea about the actual quality of care, it only tells you if more or less people are dying at your hospital compared to another hospital.
Quality is the actual clinical outcome, the treatment of the 'disease' and the patient well being, does the patient leave the hospital in a condition comparable to how he/she was before getting the 'disease'?
A great idea that came out was to use the percentage of patients that returned for follow up as a surrogate for quality, and they are investigating that now.
One way you can indirectly determine quality of care is by using patient forums (groups of patients meeting together), or using patient questionnaires. Many points that are raised by patient forums are simple and often overlooked. One group of patients who had urological operations, noted how they all had no idea what underwear to wear. It may sound stupid to the consultant who is focusing on defeating the cancer being treated (yes the true priority), but the underwear was important to the patient and the source of a great deal of stress.
"If you improve the little things the cancer becomes just a little less important"
The quality care programme at the hospital is a relatively new concept and has taken a very long time to be adopted. Apparently it took about 7 months to get a group of 20 people to talk together, 20 people all involved in different parts of the patients care pathway; nurses, doctors, physiotherapists, radiologists etc.
Communication is a big issue if you want to work on improving quality.
Unfortunately many doctors didn't appreciate advice from the nursing staff at the start, it took a long time for this communication loop to open up. Doctors interpreted the advice as nurses telling the doctors how to do their job, hostile thinking. Just because you’ve done something for 20 years doesn’t mean it is right or couldn’t be better.
Once the problem of communication is solved, drastic changes are seen. The benefits are seen not only among the hospital staff. Patient counselling groups offered to all the patients undergoing prostate cancer resection, were very popular. Patients spoke in a large group with all the staff involved in their care. Hearing about all the people going through the same problem was incredibly enlightening for the patients, even if it regarded embarrassing topics like sexual life after surgery. Understanding the process and what life is like around and after the surgery was helpful. Clinical outcomes were even seen to improve, for example continence after prostate resection was improved. Well prepared patients took their pelvic floor muscle training before surgery seriously, understanding the importance and hearing from other patients.
The quality care team started their approach with observation. They took doctors along and tried to be patients, from the start of the process to the very end. Starting from the parking lot straight away they realised why the little things are important, they couldn't even find the department, there were no signs! We need to take care of patients from the very beginning.
Their are little things you can do that can have a massive impact on patient outcomes and quality of care. Two small examples of changes at our hospital that improved quality of care:
- When a stroke victim is on the way to the hospital emergency department in the ambulance the neurologist is called before and is ready at the door when the patient arrives. as apposed to waiting ten minutes for the neurologist to arrive who has been called only on patient arrival. Time is brain after all. The Dr waits for the patient the patient doesn't have to wait.
- A case manager, who calls patients and organises their follow ups with them on the phone as apposed to the normal "see so and so after six months for ct scan" etc. speaking directly with the patient you can assure they book an appointment and also it fits around them.
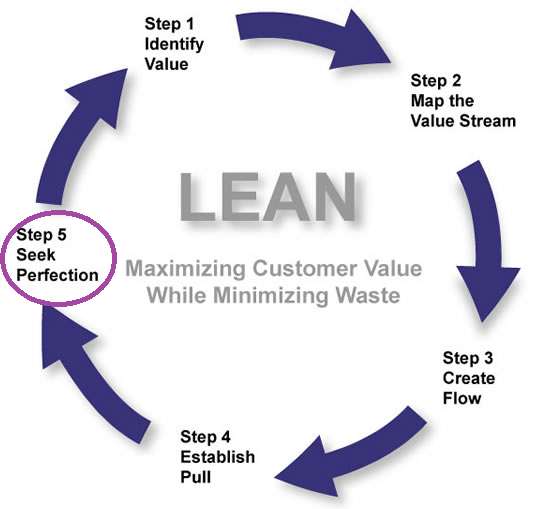
Some of the hospitals ideas came from the famous Toyota LEAN method which you can find out about in this interesting BBC discovery podcast:
http://www.bbc.co.uk/programmes/p042k1bfQuality is the actual clinical outcome, the treatment of the 'disease' and the patient well being, does the patient leave the hospital in a condition comparable to how he/she was before getting the 'disease'?
A great idea that came out was to use the percentage of patients that returned for follow up as a surrogate for quality, and they are investigating that now.
One way you can indirectly determine quality of care is by using patient forums (groups of patients meeting together), or using patient questionnaires. Many points that are raised by patient forums are simple and often overlooked. One group of patients who had urological operations, noted how they all had no idea what underwear to wear. It may sound stupid to the consultant who is focusing on defeating the cancer being treated (yes the true priority), but the underwear was important to the patient and the source of a great deal of stress.
"If you improve the little things the cancer becomes just a little less important"
The quality care programme at the hospital is a relatively new concept and has taken a very long time to be adopted. Apparently it took about 7 months to get a group of 20 people to talk together, 20 people all involved in different parts of the patients care pathway; nurses, doctors, physiotherapists, radiologists etc.
Communication is a big issue if you want to work on improving quality.
Unfortunately many doctors didn't appreciate advice from the nursing staff at the start, it took a long time for this communication loop to open up. Doctors interpreted the advice as nurses telling the doctors how to do their job, hostile thinking. Just because you’ve done something for 20 years doesn’t mean it is right or couldn’t be better.
Once the problem of communication is solved, drastic changes are seen. The benefits are seen not only among the hospital staff. Patient counselling groups offered to all the patients undergoing prostate cancer resection, were very popular. Patients spoke in a large group with all the staff involved in their care. Hearing about all the people going through the same problem was incredibly enlightening for the patients, even if it regarded embarrassing topics like sexual life after surgery. Understanding the process and what life is like around and after the surgery was helpful. Clinical outcomes were even seen to improve, for example continence after prostate resection was improved. Well prepared patients took their pelvic floor muscle training before surgery seriously, understanding the importance and hearing from other patients.
The quality care team started their approach with observation. They took doctors along and tried to be patients, from the start of the process to the very end. Starting from the parking lot straight away they realised why the little things are important, they couldn't even find the department, there were no signs! We need to take care of patients from the very beginning.
Their are little things you can do that can have a massive impact on patient outcomes and quality of care. Two small examples of changes at our hospital that improved quality of care:
- When a stroke victim is on the way to the hospital emergency department in the ambulance the neurologist is called before and is ready at the door when the patient arrives. as apposed to waiting ten minutes for the neurologist to arrive who has been called only on patient arrival. Time is brain after all. The Dr waits for the patient the patient doesn't have to wait.
- A case manager, who calls patients and organises their follow ups with them on the phone as apposed to the normal "see so and so after six months for ct scan" etc. speaking directly with the patient you can assure they book an appointment and also it fits around them.
Some of the hospitals ideas came from the famous Toyota LEAN method which you can find out about in this interesting BBC discovery podcast:
No comments:
Post a Comment