Saturday, 20 May 2017
Vinnie Jones advert for British Heart Foundation - Superb
If some geezer collapses infronta ya, what do you do?
Wednesday, 17 May 2017
Lacerations in the ER Part 1: Before you stitch!
Here are my notes from the 'Advanced wound care' lecture, the last lecture before graduation. After just an hour with this prof I felt like I could handle any laceration that comes into the ER. Hopefully after this post you will feel a similar confidence:
History is important!
Before touching the wound, you should know exactly how it happened, when it happened and what instrument/surface cause the laceration. Its important because wounds heal differently and are devitalised in many different ways depending on these factors.
Location is relevant, the face heals better than the hands. Some areas are more mobile and better perfused.
Patient factors;
Patient factors will affect healing and can be important clues for risk of infection (diabetes), healing time etc.
Steroids slow healing, HIV doesnt affect wound healing, Keloids are common in afro-americans.
Find out the patient's Tetanus Status, you have probably heard about tetanus prone wounds, this is a myth. You can get tetanus from a corneal abrasion. Make you sure you find out about the primary series of vaccinations! no good giving a booster if someone hasn't had their primary series! this is a common situation with immigrants in our ER. Many people forget to ask! CDC advice
The key to good wound practice is IRRIGATION. rememeber: "the solution to pollution is dilution" Water is the best irrigant, you can use plain old tap water, its the volume that matters, taking the patient over to the tap you can supply much more water than a simple syringe from a saline bag. You will never completely eliminate the bacteria, it just needs to have a lower enough concentration so that colonies don't form (sample principle as the lab). Consider the environment, kid falls and hits head on table legvs kid who falls and hits head on road kerb. You need volume and pressure
Sensation:
The gold standard to test sensation is a 2 point discrimination (5mm apart for the hands), make sure there eyes are closed of course. A plastic surgeon can repair most nerves proximal to the DIP joint of the fingers, you will need them to fix any nerve injuries. From a malpractice point of view you need to perform the gold standard.
You can investigate tendon injuries in a variety of ways, a good way to test is to ask the patient to assume the position of function, you will spot any flexor injuries easily.
Position of function: arms raised to shoulder height, with hands pointing up and open chest position. imagine a policeman says "hands up!"
Flexor injuries you should call the surgeon. There is a small no mans land, the deep palmar lacerations. If the palm hurts when they move their hand then they have probably knicked the palmar sheath. With little pain you can probably leave this but a surgical referral is probably best.
Many extensor tendon injuries can be splinted and will heal well.
Remove foreign bodies. 90% of glass can be seen on X-ray
Use anaesthetic, local anaesthesia or nerve block. nerve blocks are very useful and with ultrasound very easy to perform (with practice). Use Lidocaine (short acting) or Bupivicaine (medium acting 8hours half life). Some areas are tender, for example the sole of the foot, do a nerve block!
Allergic reactions to lidocaine itself are impossible! (only to the preservatives used within, which are rare now). You can be almost 100% sure there will be no allergic reaction if you use single use vials or cardiac lidocaine.
There has never ever been a documented case of allergci reaction to cardiac lidocaine.
Most lidocaine reactions are just a vasovagal reaction to the needle ha.
When dealing with the face or kids, topical agents are great eg. Tetracaine. You can wack it on in triage.
Explore all Wounds!
Anaesthesia, Betadine on the neighbouring skin surface (not inside the wound). you are ready to suture!
SUMMARY:
History is important!
Before touching the wound, you should know exactly how it happened, when it happened and what instrument/surface cause the laceration. Its important because wounds heal differently and are devitalised in many different ways depending on these factors.
Location is relevant, the face heals better than the hands. Some areas are more mobile and better perfused.
Patient factors;
Patient factors will affect healing and can be important clues for risk of infection (diabetes), healing time etc.
Steroids slow healing, HIV doesnt affect wound healing, Keloids are common in afro-americans.
Find out the patient's Tetanus Status, you have probably heard about tetanus prone wounds, this is a myth. You can get tetanus from a corneal abrasion. Make you sure you find out about the primary series of vaccinations! no good giving a booster if someone hasn't had their primary series! this is a common situation with immigrants in our ER. Many people forget to ask! CDC advice
The key to good wound practice is IRRIGATION. rememeber: "the solution to pollution is dilution" Water is the best irrigant, you can use plain old tap water, its the volume that matters, taking the patient over to the tap you can supply much more water than a simple syringe from a saline bag. You will never completely eliminate the bacteria, it just needs to have a lower enough concentration so that colonies don't form (sample principle as the lab). Consider the environment, kid falls and hits head on table legvs kid who falls and hits head on road kerb. You need volume and pressure
Sensation:
The gold standard to test sensation is a 2 point discrimination (5mm apart for the hands), make sure there eyes are closed of course. A plastic surgeon can repair most nerves proximal to the DIP joint of the fingers, you will need them to fix any nerve injuries. From a malpractice point of view you need to perform the gold standard.
You can investigate tendon injuries in a variety of ways, a good way to test is to ask the patient to assume the position of function, you will spot any flexor injuries easily.
Position of function: arms raised to shoulder height, with hands pointing up and open chest position. imagine a policeman says "hands up!"
Flexor injuries you should call the surgeon. There is a small no mans land, the deep palmar lacerations. If the palm hurts when they move their hand then they have probably knicked the palmar sheath. With little pain you can probably leave this but a surgical referral is probably best.
Many extensor tendon injuries can be splinted and will heal well.
Remove foreign bodies. 90% of glass can be seen on X-ray
Use anaesthetic, local anaesthesia or nerve block. nerve blocks are very useful and with ultrasound very easy to perform (with practice). Use Lidocaine (short acting) or Bupivicaine (medium acting 8hours half life). Some areas are tender, for example the sole of the foot, do a nerve block!
Allergic reactions to lidocaine itself are impossible! (only to the preservatives used within, which are rare now). You can be almost 100% sure there will be no allergic reaction if you use single use vials or cardiac lidocaine.
There has never ever been a documented case of allergci reaction to cardiac lidocaine.
Most lidocaine reactions are just a vasovagal reaction to the needle ha.
When dealing with the face or kids, topical agents are great eg. Tetracaine. You can wack it on in triage.
Explore all Wounds!
Anaesthesia, Betadine on the neighbouring skin surface (not inside the wound). you are ready to suture!
SUMMARY:
- History of injury
- Location considerations
- Pateint factors
- Tetanus status
- Good neurovascular and functional exam
- Irrigation
- Anaesthesia
 |
| Get ready to stitch this guy up |
Monday, 15 May 2017
An Incredibly Trippy History of the World
I actually learnt so much from this video! Although unbearably trippy it is actually really entertaining and surprisingly accurate. hats off to Bill Wurtz for this creation.
Sunday, 14 May 2017
Quality Improvement in Hospital
These notes are based on a wonderful lecture I had today titled 'quality improvement in health care pathways'. It was a short lecture full of simple but powerful ideas.
I am quite fortunate that my hospital is modern and has a lot of money. One of the ways the administration has decided to spend this money is on a 'quality care' unit whose job is simply to improve patient outcomes and increase the 'quality' of care.
Quality is notoriously difficult in healthcare to measure. The main way that quality is measured in most institutions is by comparison to local and national mortality and infection rates. Yet these gives you no idea about the actual quality of care, it only tells you if more or less people are dying at your hospital compared to another hospital.
Quality is the actual clinical outcome, the treatment of the 'disease' and the patient well being, does the patient leave the hospital in a condition comparable to how he/she was before getting the 'disease'?
A great idea that came out was to use the percentage of patients that returned for follow up as a surrogate for quality, and they are investigating that now.
One way you can indirectly determine quality of care is by using patient forums (groups of patients meeting together), or using patient questionnaires. Many points that are raised by patient forums are simple and often overlooked. One group of patients who had urological operations, noted how they all had no idea what underwear to wear. It may sound stupid to the consultant who is focusing on defeating the cancer being treated (yes the true priority), but the underwear was important to the patient and the source of a great deal of stress.
"If you improve the little things the cancer becomes just a little less important"
The quality care programme at the hospital is a relatively new concept and has taken a very long time to be adopted. Apparently it took about 7 months to get a group of 20 people to talk together, 20 people all involved in different parts of the patients care pathway; nurses, doctors, physiotherapists, radiologists etc.
Communication is a big issue if you want to work on improving quality.
Unfortunately many doctors didn't appreciate advice from the nursing staff at the start, it took a long time for this communication loop to open up. Doctors interpreted the advice as nurses telling the doctors how to do their job, hostile thinking. Just because you’ve done something for 20 years doesn’t mean it is right or couldn’t be better.
Once the problem of communication is solved, drastic changes are seen. The benefits are seen not only among the hospital staff. Patient counselling groups offered to all the patients undergoing prostate cancer resection, were very popular. Patients spoke in a large group with all the staff involved in their care. Hearing about all the people going through the same problem was incredibly enlightening for the patients, even if it regarded embarrassing topics like sexual life after surgery. Understanding the process and what life is like around and after the surgery was helpful. Clinical outcomes were even seen to improve, for example continence after prostate resection was improved. Well prepared patients took their pelvic floor muscle training before surgery seriously, understanding the importance and hearing from other patients.
The quality care team started their approach with observation. They took doctors along and tried to be patients, from the start of the process to the very end. Starting from the parking lot straight away they realised why the little things are important, they couldn't even find the department, there were no signs! We need to take care of patients from the very beginning.
Their are little things you can do that can have a massive impact on patient outcomes and quality of care. Two small examples of changes at our hospital that improved quality of care:
- When a stroke victim is on the way to the hospital emergency department in the ambulance the neurologist is called before and is ready at the door when the patient arrives. as apposed to waiting ten minutes for the neurologist to arrive who has been called only on patient arrival. Time is brain after all. The Dr waits for the patient the patient doesn't have to wait.
- A case manager, who calls patients and organises their follow ups with them on the phone as apposed to the normal "see so and so after six months for ct scan" etc. speaking directly with the patient you can assure they book an appointment and also it fits around them.
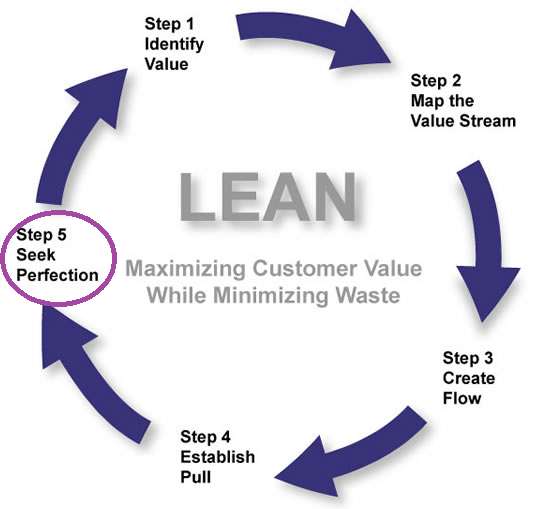
Some of the hospitals ideas came from the famous Toyota LEAN method which you can find out about in this interesting BBC discovery podcast:
http://www.bbc.co.uk/programmes/p042k1bfQuality is the actual clinical outcome, the treatment of the 'disease' and the patient well being, does the patient leave the hospital in a condition comparable to how he/she was before getting the 'disease'?
A great idea that came out was to use the percentage of patients that returned for follow up as a surrogate for quality, and they are investigating that now.
One way you can indirectly determine quality of care is by using patient forums (groups of patients meeting together), or using patient questionnaires. Many points that are raised by patient forums are simple and often overlooked. One group of patients who had urological operations, noted how they all had no idea what underwear to wear. It may sound stupid to the consultant who is focusing on defeating the cancer being treated (yes the true priority), but the underwear was important to the patient and the source of a great deal of stress.
"If you improve the little things the cancer becomes just a little less important"
The quality care programme at the hospital is a relatively new concept and has taken a very long time to be adopted. Apparently it took about 7 months to get a group of 20 people to talk together, 20 people all involved in different parts of the patients care pathway; nurses, doctors, physiotherapists, radiologists etc.
Communication is a big issue if you want to work on improving quality.
Unfortunately many doctors didn't appreciate advice from the nursing staff at the start, it took a long time for this communication loop to open up. Doctors interpreted the advice as nurses telling the doctors how to do their job, hostile thinking. Just because you’ve done something for 20 years doesn’t mean it is right or couldn’t be better.
Once the problem of communication is solved, drastic changes are seen. The benefits are seen not only among the hospital staff. Patient counselling groups offered to all the patients undergoing prostate cancer resection, were very popular. Patients spoke in a large group with all the staff involved in their care. Hearing about all the people going through the same problem was incredibly enlightening for the patients, even if it regarded embarrassing topics like sexual life after surgery. Understanding the process and what life is like around and after the surgery was helpful. Clinical outcomes were even seen to improve, for example continence after prostate resection was improved. Well prepared patients took their pelvic floor muscle training before surgery seriously, understanding the importance and hearing from other patients.
The quality care team started their approach with observation. They took doctors along and tried to be patients, from the start of the process to the very end. Starting from the parking lot straight away they realised why the little things are important, they couldn't even find the department, there were no signs! We need to take care of patients from the very beginning.
Their are little things you can do that can have a massive impact on patient outcomes and quality of care. Two small examples of changes at our hospital that improved quality of care:
- When a stroke victim is on the way to the hospital emergency department in the ambulance the neurologist is called before and is ready at the door when the patient arrives. as apposed to waiting ten minutes for the neurologist to arrive who has been called only on patient arrival. Time is brain after all. The Dr waits for the patient the patient doesn't have to wait.
- A case manager, who calls patients and organises their follow ups with them on the phone as apposed to the normal "see so and so after six months for ct scan" etc. speaking directly with the patient you can assure they book an appointment and also it fits around them.
Some of the hospitals ideas came from the famous Toyota LEAN method which you can find out about in this interesting BBC discovery podcast:
Monday, 8 May 2017
A Brief History of Stroke
Stroke is a leading global cause of death and
disability-adjusted life years (DALYs, see below for definition), second only to ischemic heart disease. The incidence of stroke varies across different countries and
increases exponentially with age.


First defined as ‘apoplexy’ by the
father of medicine Hippocrates himself in 2400BC, it was not until around the
1600’s that the link between the potentially devastating sudden symptoms and
the brain was made (hence the name ‘apoplexy’, which meant in Greek ‘struck
down by sudden violence’). This discovery was made by the documentation of
intracranial haemorrhage in the brains of cadavers who died of stroke by
Johannes Wepfer (Since 2005 the “Johann Jacob Wepfer Award” is given at the
European Stroke Conference for outstanding work in cerebrovascular diseases).


After extensive work in defining the anatomy of the cerebral vasculature by
Thomas Willis in Oxford 1664, and the discovery of an anatomo-pathological
association by the Paris Medical School in the late 1800s, apoplexy became
better known as ‘cerebrovascular accident’. The term ‘stroke’ was a lay term, originating
from the belief the disease was a sort of ‘stroke of gods hand’ or ‘stroke of
justice’, a punishment for wrongdoing or pleasure-seeking. It later became the
definitive name for the disease in 1962 when the chest and heart association
produced a booklet titled ‘Modern Views
on ‘Stroke’ Illness’.
Even at this time, the mid twentieth century, it seemed
doctors still approached stroke with slight nihilism or hopelessness. Up until
1935 bloodletting was the primary therapy for stroke. Vomits, purges and enemas
were all treatments for stroke in the beginning of the nineteenth century, not
so different from Hippocrates own ‘replacement of humours’ before the start of
the millennium. Nothing seemed to improve the prognosis, patients miraculously
recovered, died or faded away with permanent disability; modern medicine had a
long way to go still!
 |
| Bloodletting, 'back in the day' |
In the 1950s doctors began to experiment with angiography,
anticoagulants and surgery for the treatment of stroke. A few years later, team
approaches to stroke patients started in many hospitals with the collaboration
of physiotherapists, nurses, dietitians, surgeons, internists, occupational
therapists, speech therapists and general practitioners. Rehabilitation became
one of the main contemporary treatment responses to stroke. By the end of the
20th century and with birth of stroke associations around the world,
there seemed to be some light in the tunnel, perhaps stroke is curable and
preventable.
Stroke treatment and management has come a long way in the last
fifty years, advancements in angiography and the introduction of aspirin
therapy and intravenous thrombolysis have improved survival massively.
In 2008,
stroke moved from being the 3rd leading cause of death in the USA to
the fourth, it then jumped a further rank to fifth in 2013, a reflection of
accelerating science and improving prognosis!
DALY: The sum of years of
potential life lost due to premature mortality and the years of productive life lost
due to disability. One DALY can be thought of as
one lost year of "healthy" life. The sum of these DALYs across the
population, or the burden of disease, can be thought of as a measurement of the
gap between current health status and an ideal health situation where the
entire population lives to an advanced age, free of disease and disability.
References:
-http://vizhub.healthdata.org/gbd-compare/
Institute for health metrics and evaluation. Accessed 03/04/2017. Images.
-Catherine E. Storey, Hans Pols, Chapter 27 A history of cerebrovascular disease, In: Michael J. Aminoff, François Boller and Dick F. Swaab, Editor(s), Handbook of Clinical Neurology, Elsevier, 2009, Volume 95, Pages 401-415, ISSN 0072-9752, ISBN 9780444520098, http://dx.doi.org/10.1016/S0072-9752(08)02127-1.
-Molnár
Z. Thomas Willis (1621-1675), the founder of clinical neuroscience. Nat Rev
Neurosci. 2004;5(4):329-35.
-Van der worp HB, Van gijn J. Clinical practice. Acute ischemic stroke. N Engl J Med. 2007;357(6):572-9.
-Pound P, Bury M, Ebrahim S. From apoplexy to stroke. Age Ageing. 1997;26(5):331-7.
Friday, 5 May 2017
Monday, 1 May 2017
If BY RUDYARD KIPLING
If you can keep your head when all about you
Are losing theirs and blaming it on you,
If you can trust yourself when all men doubt you,
But make allowance for their doubting too;
If you can wait and not be tired by waiting,
Or being lied about, don’t deal in lies,
Or being hated, don’t give way to hating,
And yet don’t look too good, nor talk too wise:
If you can dream—and not make dreams your master;
If you can think—and not make thoughts your aim;
If you can meet with Triumph and Disaster
And treat those two impostors just the same;
If you can bear to hear the truth you’ve spoken
Twisted by knaves to make a trap for fools,
Or watch the things you gave your life to, broken,
And stoop and build ’em up with worn-out tools:
If you can make one heap of all your winnings
And risk it on one turn of pitch-and-toss,
And lose, and start again at your beginnings
And never breathe a word about your loss;
If you can force your heart and nerve and sinew
To serve your turn long after they are gone,
And so hold on when there is nothing in you
Except the Will which says to them: ‘Hold on!’
If you can talk with crowds and keep your virtue,
Or walk with Kings—nor lose the common touch,
If neither foes nor loving friends can hurt you,
If all men count with you, but none too much;
If you can fill the unforgiving minute
With sixty seconds’ worth of distance run,
Yours is the Earth and everything that’s in it,
And—which is more—you’ll be a Man, my son!

Subscribe to:
Posts (Atom)