
Saturday, 30 April 2016
Tuesday, 26 April 2016
Monday, 25 April 2016
Children are not little adults
Starting Paediatrics today, its important to realize that the medical approach to children can be incredibly different than that to adults. Children differ from adults physiologically and in their exposure to the environment, here is a list of some important points to consider when dealing with a paediatric patient:
(this post is based on the WHO document linked here, reference are included within that document)
In summary, children have unique and differing-to-adults exposures and a highly dynamic developmental physiology. Combining this with a longer life expectancy and the insidious effects of environmental toxins, it is very important to consider the world/environment we leave behind for children to inherit.
Children have a completely different pharmacokinetic profile and can be exposed in a variety of ways, so its also important for physicians to be vigiliant in paediatrics pharmo-prescribing.
Bonus point: Introducing a food early to children does not increase their risk of allergies, NEJM editorial.

(this post is based on the WHO document linked here, reference are included within that document)
- Minute ventilation per Kg bodyweight a day is higher in children. It is around 600l in <1year old which is 3 times the value of an adult, 200l. Therefore environmental toxicants will be delivered to the airways of a child at a higher level than adults. for example: ozone, lead, particulates, nitrogen oxides, mercury, moulds, volatile organic compunds etc.
- Calorie and water needs are higher in children. Cal/kg/day and ml/kg/day have higher values in younger children, its pretty obvious considering their anabolic state and growth demands. Therefore oral exposures are likely to be higher in children, think of pesticides or mycotoxins that are common in food. I could mention here that a vegan diet may be harmful to children since their calorie demand is so much higher (even though I'm an avid supporter of plant based diets).
- Gastrointestinal absorption is higher in children and dynamic. For example a child may absorb 70% of ingested lead while an adult around 5-20%. There are microbiome changes throughout childhood, contributing to digestion and absorption. important considering pharmacokinetics, always prescribe drugs in mg/kg not by single doses.
- Renal function: GFR (glomerular filtration rate) is low at birth (around 10-15ml/min/m2 for a normal full term newborn) and doubles in the first week of life (cirtical period). GFR reaches adult values by around 6-12 months, the general rule is 8 months. tubular function is impaired (secretion) at birth and is normal by 1 year of life.
- Hepatic function: The activity of phase 1 enzymes are reduced and mature at different rates as child grows. in fact activity of these enzymes can then exceed adult rates between 6-12 years age. phase two enzymes are ready at birth for processes such as conjugation and acetylation. Therefore metabolites of xenobiotics may differ between adults and children, even if rates of metabolism are the same.
- Transplacental exposures: Many chemicals and drugs cross the placenta, including mercury, lead, substances of abuse, alcohol etc. We all know the story of thalidomide. Also physical factors can affect the baby such as heat and ionizing radiation. important thing to point out here is that maternal exposures do matter!
- Breastfeeding: Breast milk is the safest and most complete nutrition for infants, so mothers should avoid toxic exposures. We use breast milk to spot environmental contaminants, its very likely that you reading this have DDT in your fat because your mother was exposed to it as a child. Lipophilic chemicals are especially good at transferring in breast milk, hence why we don't prescribe quinolones for breastfeeding mothers.
- Size and surface area: The ratio between skin/surface area to body volume/mass is much higher in children, about 3x for a newborn compared to an adult and 2 times with an infant. therefore dermal exposures may be much higher in children, children also tend to have more skin abrasions/cuts and rashes which make it easier for germs/contaminants to cross the skin barrier. Very important to consider the surface area in children when dealing with burns.
- Organ and system development: the organs in a childs bodie grow and mature throughout childhood. Neuron growth and maturation (myelination and synpatogenesis) continues right the way through puberty, The respiratory system continues linear growth after birth so any exposures to toxic compunds (tobacco smoke! ozone etc.) can have very adverse consequences. The immune system is also actively maturing throughout childhood.
In summary, children have unique and differing-to-adults exposures and a highly dynamic developmental physiology. Combining this with a longer life expectancy and the insidious effects of environmental toxins, it is very important to consider the world/environment we leave behind for children to inherit.
Children have a completely different pharmacokinetic profile and can be exposed in a variety of ways, so its also important for physicians to be vigiliant in paediatrics pharmo-prescribing.
Bonus point: Introducing a food early to children does not increase their risk of allergies, NEJM editorial.

Sunday, 24 April 2016
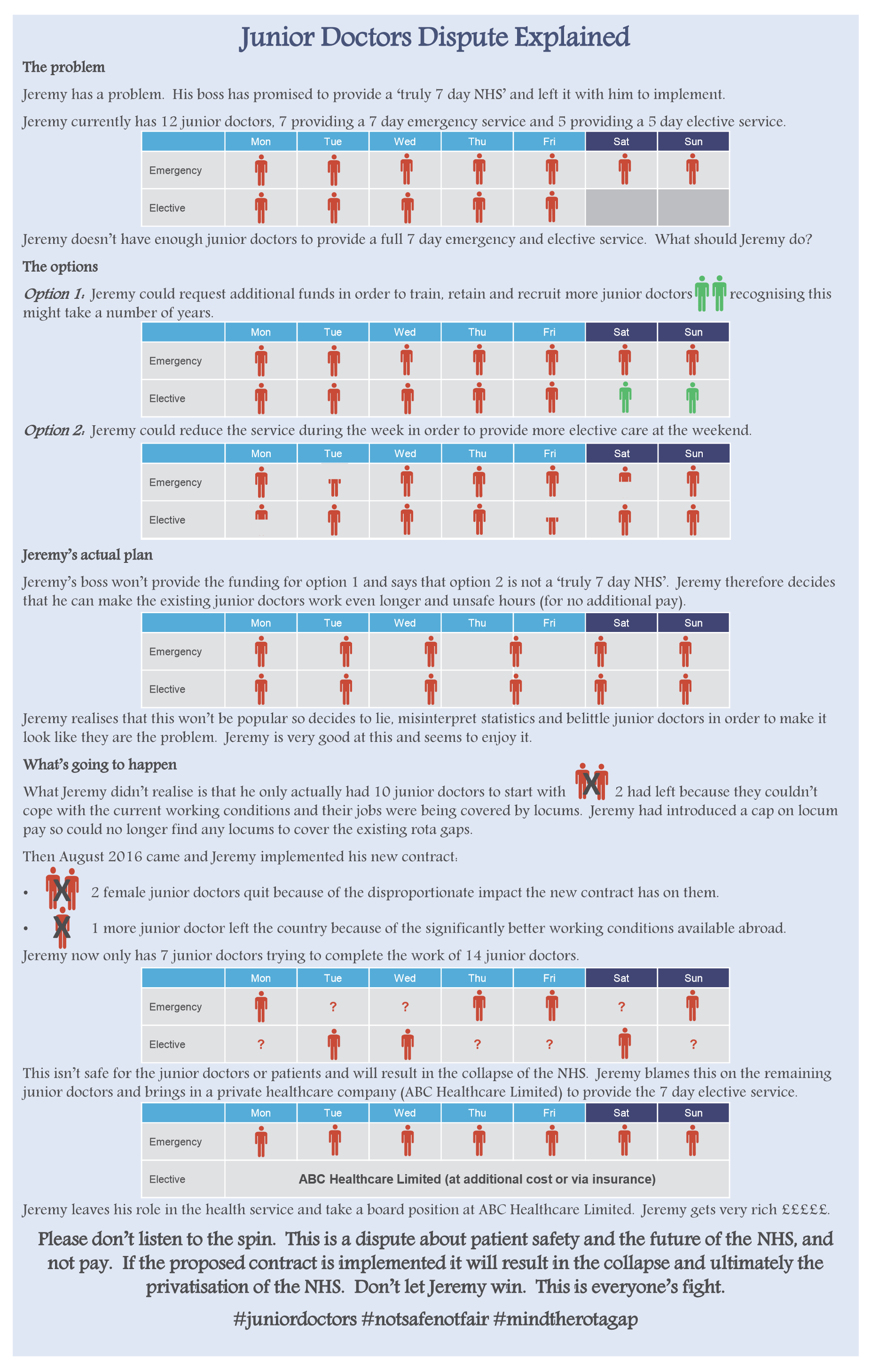
Junior doctors dispute explianed
This explains well the juniors doctors point of view with the current contract dispute.
http://imagizer.imageshack.us/a/img922/3550/F1r5so.png

http://imagizer.imageshack.us/a/img922/3550/F1r5so.png
{kind=link}

Saturday, 23 April 2016
So you want to learn a new language...
Today is the United nations world English Language Day So I've decided to share the many methods I used to learn italian, that should apply to learning any language (even English).
First of all before even considering the list below, hands down the best way to learn any language is to live in a country and with the people that speak that language.
Here a list of what I use to learn languages:

First of all before even considering the list below, hands down the best way to learn any language is to live in a country and with the people that speak that language.
Here a list of what I use to learn languages:
- Babbel: costs a little but offers a comprehensive course for many languages at all levels, i got a super cheap membership with so random GroupOn deal, anyway moving on.
- Duolingo: its completely free! this app is great to practise the basics, you can even compete with friends.
- Grammar books: the back bone of learning grammar is practise, find a textbook like this just full of simple exercises.
- Dual language books: in my opinion utterly useless, but I didn't stop me using them for many years.
- Skype language exchanges: Tandem is particularly good, also heard about Hellotalk.
- Blogs: there are absolutely millions of language blogs, you have to sift through them to find a good one like this and this, best of all they are completely free!
- Podcasts: this coffeebreak series by radiolingua is incredible and again freeeee!
You dont have to spend any money to learn a language it only requires dedication and of course hours of practise practise practise.
I found this book really helped, Fluent Forever by Gabriel Wyner.

Thursday, 21 April 2016
Creativity, it's more than practise
Summary and interpretation of this interesting article by Scientific American on creativity.
Creativity doesn't fit the old adage of 'practise makes perfect' or deliberate practise. It needs to be original, meaningful and surprising (as defined by the US patent office). Here are some tips and realities about creativity:
"I hope I have convinced you that creators are not mere experts. Creativity does draw on a deep knowledge base, and delibrate practice can certainly contribute to many aspects of creativity, but ultimately creativity involves much more than just deliberate practice. Creators are not necessarily the most efficient, but their messy minds and messy processes often allow them to see things others have never seen, and to create new paths that future generations will deliberately practice."

Creativity doesn't fit the old adage of 'practise makes perfect' or deliberate practise. It needs to be original, meaningful and surprising (as defined by the US patent office). Here are some tips and realities about creativity:
- Creativity is blind: often luck plays a role
- Creative people often have messy processes: your most creative work may come before your worst piece of work, it can be random.
- Creators rarely receive helpful feedback: standards are constantly changing, so you cant rely on feedback.
- The 'ten year rule' doesn't apply to creativity: you don't need ten years to become an expert as in many trainable skills, but time does help.
- Talent isn't relevant: talent is simply 'the rate that someone gains expertise', since expertise isn't always required it isn't necessary. talent will help a creator learn what already exists.
- Personality is relevant: creators tend to have a more independent, unconformity, risk taking and unconventionality based personality. They also tend to be more open to new experiences.
- Genes are relevant: genes determine personality and behaviour
- Environment also plays a role: perhaps the biggest conrtibutor to creativity, look for a new environment and a great mentor.
- Creative people have broader interests and more versatility: cross hobbies, dont focus on one occupation/topic/pasttime.
- Too much expertise can be detrimental to creativity: for example learning everything there is to know about creative writing will limit your creative writing ability in terms of creativity (counter-intiutive I know)
- Outsiders often have the creative advantage
"I hope I have convinced you that creators are not mere experts. Creativity does draw on a deep knowledge base, and delibrate practice can certainly contribute to many aspects of creativity, but ultimately creativity involves much more than just deliberate practice. Creators are not necessarily the most efficient, but their messy minds and messy processes often allow them to see things others have never seen, and to create new paths that future generations will deliberately practice."
-Scott Barry Kaufman

Tuesday, 12 April 2016
Quote of the day: Elisa Ottensen-Jenson

Video: Why Did Mrs X Die, Retold
WHO factsheet for maternal mortality.
Fortunately Maternal health is one of the United nations sustainable dvelopment goals, Hopefully will see some change of the next few years.
Monday, 11 April 2016
Dont waste your BREXIT vote
On the 23rd of June a referendum will be held in the UK to decide whether Britain should stay in the EU or leave (Brexit). Leaving the EU will put restrictions on free trade, free movement of labour and affect our global trading power (as well as security, believe it not). Brexit will be a nightmare for expats abroad and students like myself studying in Europe (because of restriction of free movement, VISA, taxes etc).
Admittedly the statistic that Britain pays more than they get back is true in terms of hard cash but if they were no longer in the EU that difference would be much larger. Of course the actual effects of Brexit or staying in will all vary depending on the deal that is made with the EU after the voting.
A good explanation by the BBC linked here.
This link shows you how you can vote while abroad. I for one will be rushing to make sure I get my vote in, as BREXIT will be bad news for me, a student abroad. UK governments own advice link.

Admittedly the statistic that Britain pays more than they get back is true in terms of hard cash but if they were no longer in the EU that difference would be much larger. Of course the actual effects of Brexit or staying in will all vary depending on the deal that is made with the EU after the voting.
A good explanation by the BBC linked here.
This link shows you how you can vote while abroad. I for one will be rushing to make sure I get my vote in, as BREXIT will be bad news for me, a student abroad. UK governments own advice link.

Sunday, 10 April 2016
April round-up (Medical student gems)
Youtube Channel: theedexitvideo
TheEDexitvideo channel run by Dr Carlo Oller gives great insight into life as an emergency department physician. It's a wonderful educational resource with the personal touch of a real down to earth honest doc.
Book: How Not to Die
Dr Michael Gregers book has been a long time in the works. Finally released last autumn, how not to die is a must read for anybody with an interest in nutrition. It even got me munching on plants more often.
Twitter accounts: @HansRosling @ShaunLintern
Professor of global health at the Karolinska institute, creator of Gapminder.org and the Gapminder foundation, Hans Rosling. Sign up for his entirely free online introduction to global health course at eDX. Shaun Lintern a patient safety correspondent and a good one to follow to keep in touch with various issues with the UK health system.
Webpage: Global burden of disease
This interactive website run by the Institute for Health Metrics and Evaluation, is just fantastic. You can play around with the various graph styles, regions and income groups to have a really clear world view on the impact of diseases in the different groups.
Film: Sicko
This famous Michael Moore documentary looks gives insight into the drawbacks and horrors of the American health system, although slow to start it is quite shocking. His latest documentary ‘where to invade next’ flopped, however Sicko is iconic Michael Moore at his best.

TheEDexitvideo channel run by Dr Carlo Oller gives great insight into life as an emergency department physician. It's a wonderful educational resource with the personal touch of a real down to earth honest doc.
Book: How Not to Die
Dr Michael Gregers book has been a long time in the works. Finally released last autumn, how not to die is a must read for anybody with an interest in nutrition. It even got me munching on plants more often.
Twitter accounts: @HansRosling @ShaunLintern
Professor of global health at the Karolinska institute, creator of Gapminder.org and the Gapminder foundation, Hans Rosling. Sign up for his entirely free online introduction to global health course at eDX. Shaun Lintern a patient safety correspondent and a good one to follow to keep in touch with various issues with the UK health system.
Webpage: Global burden of disease
This interactive website run by the Institute for Health Metrics and Evaluation, is just fantastic. You can play around with the various graph styles, regions and income groups to have a really clear world view on the impact of diseases in the different groups.
Film: Sicko
This famous Michael Moore documentary looks gives insight into the drawbacks and horrors of the American health system, although slow to start it is quite shocking. His latest documentary ‘where to invade next’ flopped, however Sicko is iconic Michael Moore at his best.

Saturday, 9 April 2016
'I did the training, got the T-shirt, but are you willing to be your life on me?' The Medical simulation revolution
Attended a fantastic lecture by Mark Bowyer an ex
trauma and combat surgeon, now professor of surgery at Uniformed University
(where American Army doctors study medicine).
The lecture was all about the different types and benefits of medical
simulators available, particularly in surgery and combat medicine. 
An important thing about simulation is that you can allow people to fail, because well like it or not, it does happen. You can repeat interventions as many times as you like, develop goal orientated practise and use it as a teaching tool. These days most methods are expensive, (medical education is expensive in general though) but as the industry grows, hopefully we will be seeing more of it. It's a powerful tool and we are probably just entering a new age of medical education as it grows. Dr Bowyer spent the second half of the presentation describing the various methods of solution available and their pros and cons. Before starting medical school I was a simulated patient for the UK OSCE exams, I had to pretend to have various symptoms like hearing loss, blindness and at one point some respiratory condition. Simulated patients provide an optimum human experience; history taking, physical exams and re-enacted disaster scenes, you can't get much more real than dealing with a living breathing human being. Dr Bowyer had a volunteer simulated patient who had already lost his legs in battle enacting a scene that his legs were blown off with fake blood on the ends, a powerful image for new army doctors. How do you prepare someone for the 'image' of trauma.? Part task trainers is another method of simulation for example peritoneal lavage (simPL) simulation. Students can puncture a synthetic membrane (made to look like abdomen, with umbilicus etc) with a needle that is tracked on a computer screen in front, the simulator mimics the pop of crossing the fascia and the peritoneum. Another way this technique can be trained is on a pig. Animals however do not have human anatomy and a small study comparing the computerised synthetic membrane to pig for peritoneal lavage showed better site selection and seldinger technique with the synthetic model. Working with the gaming industry and virtual reality technology, there is an expanding market of surgery simulation games. Some less professional like the very entertaining Surgeon Simulator 2013 but some more more didactic and professional as Touch surgery.
Dr Bowyer showed some incredible examples of 'virtual environments', another new medium for medical simulation. In these virtual environments you can simulate sounds, smells, scenery, noise, smoke, gun fire and much more (air cannons were used to simulate bombs going off nearby). One such environment had a helicopter platform that tipped and rolled just like a real helicopter, where the soldier could simulate getting a patient aboard and then treating him/her while the helicopter 'flew'. Just check out this WAVE (wide area virtual environment) simulator: https://www.youtube.com/watch?v=ineGH9Smce0
With the enrolment of multiple actors and simulated patients, you can simulate mass casualties and disaster zone situations using this technology.
When it comes to surgery, there are already simulators available for laparascopic and robotic surgery but the real challenge is open surgery simulation. A model of open surgery needs to act like human tissue, be anatomically correct and bleed in a realistic fashion. There has already been some success with visco-elastic foam models. One such model was used to teach doctors going out to Irag the correct procedure for fasciotomies and will have saved many legs from amputation. wouldn't you rather train on a simulator before performing an amputation tomorrow?
Now there are even simulators in development for teaching c-sections to third world countries.
Medical simulation is the new revolution in medical education! hopefully we will see one day a standardized curricula based on physical models that is consensus driven, validated, proficiency-based, offers remediation strategies and assessable to all.
 |
| Cricothyroidotomy training simulator |
Sunday, 3 April 2016
Sounds of Brighton (Quantic edition)
Will Holland AKA Quantic produces his sweet latin sounds under the Brighton label Tru Thoughts, love his stuff. Perfect mix to finish up your spring cleaning too.
Saturday, 2 April 2016
Caesarean section: National Geographic infographic


Taken from national geographic April 2016 edition 'photo ark'
Subscribe to:
Comments (Atom)