If you look up the definition of acute renal failure (ARF) you will probably find this; "an abrupt and sustained decrease in renal function". Thats all very well but what do any of these words mean?! how abrupt? how long is sustained? renal function measured how? Whats more, over 35 different definitions of ARF are used in the literature with varying mortality and incidence rates. This post should hopefully clear everything up about ARF and AKI and give some tips about how to manage ARF and AKI.
First of all, scrap the term ARF, the term AKI is used now and reflects much better the fact that small decrements in organ function not resulting in organ failure are still clinically important! ARF is used for the last stage of AKI where the kidney actually fails and RRT (renal replacement therapy, for example hemodialysis) is needed.
Diagnosis:
How do you know if a patient has AKI? look at serum creatinine and urine output!
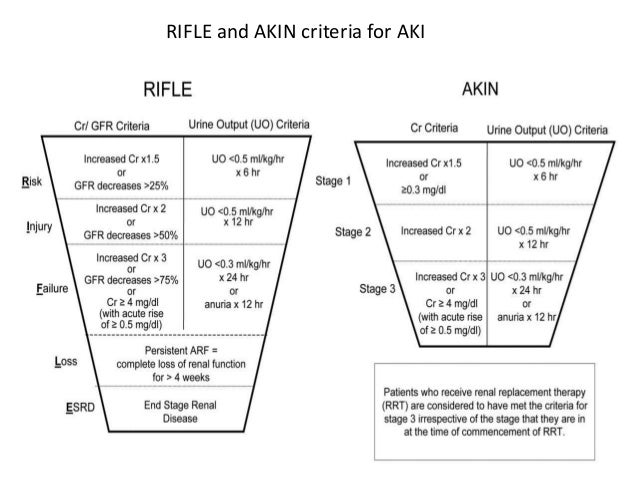
There are two main ways for classifying AKI, the RIFLE criteria and the
AKIN criteria, both perform equally well in studies, but I will use AKIN criteria because it is used by the
KDIGO guidelines which most of this post is based on.
Picture above shows the AKIN criteria in the red box, as you can see you can divide AKI into three stages depending on the level of serum creatinine (sCr) or urine output (UO) (or directly place them into stage 3 if they are on RRT or anuric for greater than 12 hours). Stage 3 AKI is synonymous with ARF.
So you have assessed your patients sCr and UO and find that he/she has an AKI. what do you do next?
AKI Management:
- monitor diuresis (bladder catheterise if not already catheterised)
- careful physical exam (pay attention to whether the patient is 'wet or dry', you should be careful giving fluids in a 'wet' pt, see later notes on pulmonary edema)
- monitor fluid balance
- arterial blood gases
- order labs: sCr, Na+, K+, Ca2+, Cl-, CBC, urine dipstick, BUN,
- renal US (you are looking for the easy dx of obstruction, see etiology below)
- CXR (pulmonary edema?)
- avoid contrast agents if at all possible
- consider ICU if stage 2 and up
- avoid hyperglycemia
- careful drug review:
- discontinue nephrotoxic drugs (eg. vancomycin, gentamycin)
- discontinue drugs that impair GFR autoregulation (NSAIDs, ACEi, ARBS(angiotension receptor blockers))
- adjust dosage of drugs undergoing renal excretion (many antibiotics)
- withhold exogenous potassium (look for K+ containing infusions (such as isolyte) that the patient may be on) and stop potassium sparing diuretics like spironolactone and eplerenone.
AKI treatment:
Treatment is mainly directed at the underlying causes, for example if the cause is dehydration give fluids, if the cause is haemorrhage consider giving blood transfusion etc. immunosuppressants for vasculitis, discontinue drugs, relieve urinary tract obstructions....
note: No specific treatment for AKI actually exists but we have to manage all the complications well.
AKI causes:
The causes of AKI are best divided into three main catergories
- pre-renal
- intrinsic (parenchymal)
- post-renal
Pre-renal AKI:
Basically anything that causes a drop in blood pressure low enough that the kidneys own auto-regulation is unable to preserve renal function. consider:
Volume loss: hemorrhage, dehydration, diarhhea, polyuria, burns
Sequestration of fluids (3rd spacing): pancreatitis, peritonitis, rhabdomyolysis
Blood pressure drop: any form of Shock, hypotensive medications
(note that not all patients have the same capacity to autoregulate their renal filtration)
Intrinsic AKI:
diseases that affect the kidney directly, consider:
Arteries: thrombosis, embolic events
Pre-glomerular arterioles: Vasculitis, malignant hypertension, atheroembolism, DIC, eclampsia
Glomeruli: glomerulonephritis, thrombotic microangiopathy
Tubulo-interstitium: Acute tubular necrosis (ATN), crystalluria, cast nephropathy, contrast agents
(note that anything that can cause a sustained hypotension can damage the renal epithelium and cause ATN)
Post-renal AKI:
This is caused by an obstruction to the urinary tract, consider:
Bladder outlet obstruction: BPH, urethra stenosis, neurologic bladder
Ureter obstruction in pts with 1 kidney: stones, cancer, papillary necrosis
AKI Complications:
AKI patients can die of four main causes:
- Hyperkalemia
- Metabolic acidosis
- Fluid accumulation (pulmonary edema)
- Uremic syndrome
Hyperkalemia occurs when serum K+ is >5 mmol/l
Symptoms of hyperkalemia include: intestinal colic, diarhee, weakness/paralysis, arthymias
Hyperkalemia has a distinct ECG: flattened P waves, wide QRS, peaked T waves
(peaked T waves is the first feature to appear)
Metabolic acidosis is caused by the failure of tubular interstutium to excrete normal daily acid load. symptoms include: nausea and vomiting, abdominal pain, hyperventilation, hypotension
(note that acidosis may worsen hyperkalemia)
Fluid accumulation is quite often iatrogenic! careful with hydration.
Uremic syndrome has many presentations and may cause: pericardial effusion, nausea and vomiting, malaise, confusion, seizures, non specific diffuse abdominal pain, ileus, a tendency to bleed (so called 'lazy' platelets).





{kind=link}